Purpose: We aim to describe the fundal fluorescein angiography (FFA) findings in a patient with COL4A1 mutation which to date has not been described in this condition. We hope to highlight the variability in ocular phenotypes seen in COL4A1 mutation, even between eyes in the same patient. Methods: Case Report. Results: A 14 year-old girl with a history of cerebral palsy, cerebral visual impairment and COL4A1 mutation with porencephaly has been attending the eye service for bilateral aphakic glaucoma with previous bilateral glaucoma tube surgery on Latanoprost, Brinzolamide and Timolol to both eyes. She developed a spontaneous right vitreous haemorrhage and anterior chamber hyphaema, subsequently requiring a vitrectomy and anterior chamber washout due to elevated intraocular pressure. Intraoperatively, she was noted to have extensive ischemic changes in the right eye. In her left fundus, there were sclerosed arterioles emanating from the disc, with the rest of the retina being normal. Despite the vitrectomy, the right eye vitreous haemorrhage and hyphaema recollected over time with persistently high intraocular pressure. She underwent a repeat vitrectomy and washout, subsequent cyclodiode laser and evisceration after she developed a painful blind right eye. During the course of her treatment, a FFA for her left eye was performed. Delay in arm-retinal time and a “fern-leaf” pattern of capillary leakage was noted. Discussion: The disease resulting from COL4A1 mutation is extremely variable. We report a patient with COL4A1 mutation with asymmetric retinal pathology with one eye eventually needing evisceration. This case highlights the need to have a high index of suspicion for early detection and asymmetric disease. There should be a low threshold for further evaluation such as FFA or optical coherence tomography (OCT) angiography to evaluate for ocular perfusion. Although COL4A1 is a systemic disease, it can have asymmetric presentation between two eyes.
| Published in | World Journal of Medical Case Reports (Volume 7, Issue 1) |
| DOI | 10.11648/j.wjmcr.20260701.11 |
| Page(s) | 1-4 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Angiogram, Col4A1, Heterogenous, Retina
FFA | Fundal Fluorescein Angiography |
OCT | Optical Coherence Tomography |
HANAC | Hereditary Angiopathy with Nephropathy, Aneurysm, and Muscle Cramps |
IOP | Intraocular Pressure |
FRAT | Familial Retinal Arteriolar Tortuosity |
| [1] | Gould DB, Phalan FC, van Mil SE, Sundberg JP, Vahedi K, Massin P, Bousser MG, Heutink P, Miner JH, Tournier-Lasserve E, John SW. Role of COL4A1 in small-vessel disease and hemorrhagic stroke. N Engl J Med. 2006 Apr 6; 354(14): 1489-96. |
| [2] | Breedveld G, de Coo IF, Lequin MH, Arts WF, Heutink P, Gould DB, John SW, Oostra B, Mancini GM. Novel mutations in three families confirm a major role of COL4A1 in hereditary porencephaly. J Med Genet. 2006 Jun; 43(6): 490-5. |
| [3] | Vahedi K, Massin P, Guichard JP, Miocque S, Polivka M, Goutières F, Dress D, Chapon F, Ruchoux MM, Riant F, Joutel A, Gaudric A, Bousser MG, Tournier-Lasserve E. Hereditary infantile hemiparesis, retinal arteriolar tortuosity, and leukoencephalopathy. Neurology. 2003 Jan 14; 60(1): 57-63. |
| [4] | Sibon I, Coupry I, Menegon P, Bouchet JP, Gorry P, Burgelin I, Calvas P, Orignac I, Dousset V, Lacombe D, Orgogozo JM, Arveiler B, Goizet C. COL4A1 mutation in Axenfeld-Rieger anomaly with leukoencephalopathy and stroke. Ann Neurol. 2007 Aug; 62(2): 177-84. |
| [5] | Plaisier E, Gribouval O, Alamowitch S, Mougenot B, Prost C, Verpont MC, Marro B, Desmettre T, Cohen SY, Roullet E, Dracon M, Fardeau M, Van Agtmael T, Kerjaschki D, Antignac C, Ronco P. COL4A1 mutations and hereditary angiopathy, nephropathy, aneurysms, and muscle cramps. N Engl J Med. 2007 Dec 27; 357(26): 2687-95. |
| [6] | Faure C, Castrale C, Benabed A, Cognard P, Lezé R, Castro-Farias D, Gérard M, Louapre C, Paques M. Structural and functional analysis of retinal vasculature in HANAC syndrome with a novel intronic COL4A1 mutation. Microvasc Res. 2023 Jan; 145: 104450. |
| [7] | Trouillet A, Lorach H, Dubus E, El Mathari B, Ivkovic I, Dégardin J, Simonutti M, Paques M, Guillonneau X, Sennlaub F, Sahel JA, Ronco P, Plaisier E, Picaud S. Col4a1 mutation generates vascular abnormalities correlated with neuronal damage in a mouse model of HANAC syndrome. Neurobiol Dis. 2017 Apr; 100: 52-61. |
| [8] | Meuwissen ME, Halley DJ, Smit LS, Lequin MH, Cobben JM, de Coo R, van Harssel J, Sallevelt S, Woldringh G, van der Knaap MS, de Vries LS, Mancini GM. The expanding phenotype of COL4A1 and COL4A2 mutations: clinical data on 13 newly identified families and a review of the literature. Genet Med. 2015 Nov; 17(11): 843-53. |
| [9] | Plaisier E, Chen Z, Gekeler F, Benhassine S, Dahan K, Marro B, Alamowitch S, Paques M, Ronco P. Novel COL4A1 mutations associated with HANAC syndrome: a role for the triple helical CB3 [IV] domain. Am J Med Genet A. 2010 Oct; 152A(10): 2550-5. |
| [10] | Jeanne M, Gould DB. Genotype-phenotype correlations in pathology caused by collagen type IV alpha 1 and 2 mutations. Matrix Biol. 2017 Jan; 57-58: 29-44. |
| [11] | Zenteno JC, Crespí J, Buentello-Volante B, Buil JA, Bassaganyas F, Vela-Segarra JI, Diaz-Cascajosa J, Marieges MT. Next generation sequencing uncovers a missense mutation in COL4A1 as the cause of familial retinal arteriolar tortuosity. Graefes Arch Clin Exp Ophthalmol. 2014 Nov; 252(11): 1789-94. |
| [12] | Alavi MV, Mao M, Pawlikowski BT, Kvezereli M, Duncan JL, Libby RT, John SW, Gould DB. Col4a1 mutations cause progressive retinal neovascular defects and retinopathy. Sci Rep. 2016 Jan 27; 6: 18602. |
APA Style
Koh, Y. T., Schmoll, C. (2026). Case Report: Asymmetric Retinal and Fundal Fluorescein Angiogram Findings in Col4A1 Mutation. World Journal of Medical Case Reports, 7(1), 1-4. https://doi.org/10.11648/j.wjmcr.20260701.11
ACS Style
Koh, Y. T.; Schmoll, C. Case Report: Asymmetric Retinal and Fundal Fluorescein Angiogram Findings in Col4A1 Mutation. World J. Med. Case Rep. 2026, 7(1), 1-4. doi: 10.11648/j.wjmcr.20260701.11
@article{10.11648/j.wjmcr.20260701.11,
author = {Yan Tong Koh and Conrad Schmoll},
title = {Case Report: Asymmetric Retinal and Fundal Fluorescein Angiogram Findings in Col4A1 Mutation},
journal = {World Journal of Medical Case Reports},
volume = {7},
number = {1},
pages = {1-4},
doi = {10.11648/j.wjmcr.20260701.11},
url = {https://doi.org/10.11648/j.wjmcr.20260701.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20260701.11},
abstract = {Purpose: We aim to describe the fundal fluorescein angiography (FFA) findings in a patient with COL4A1 mutation which to date has not been described in this condition. We hope to highlight the variability in ocular phenotypes seen in COL4A1 mutation, even between eyes in the same patient. Methods: Case Report. Results: A 14 year-old girl with a history of cerebral palsy, cerebral visual impairment and COL4A1 mutation with porencephaly has been attending the eye service for bilateral aphakic glaucoma with previous bilateral glaucoma tube surgery on Latanoprost, Brinzolamide and Timolol to both eyes. She developed a spontaneous right vitreous haemorrhage and anterior chamber hyphaema, subsequently requiring a vitrectomy and anterior chamber washout due to elevated intraocular pressure. Intraoperatively, she was noted to have extensive ischemic changes in the right eye. In her left fundus, there were sclerosed arterioles emanating from the disc, with the rest of the retina being normal. Despite the vitrectomy, the right eye vitreous haemorrhage and hyphaema recollected over time with persistently high intraocular pressure. She underwent a repeat vitrectomy and washout, subsequent cyclodiode laser and evisceration after she developed a painful blind right eye. During the course of her treatment, a FFA for her left eye was performed. Delay in arm-retinal time and a “fern-leaf” pattern of capillary leakage was noted. Discussion: The disease resulting from COL4A1 mutation is extremely variable. We report a patient with COL4A1 mutation with asymmetric retinal pathology with one eye eventually needing evisceration. This case highlights the need to have a high index of suspicion for early detection and asymmetric disease. There should be a low threshold for further evaluation such as FFA or optical coherence tomography (OCT) angiography to evaluate for ocular perfusion. Although COL4A1 is a systemic disease, it can have asymmetric presentation between two eyes.},
year = {2026}
}
TY - JOUR T1 - Case Report: Asymmetric Retinal and Fundal Fluorescein Angiogram Findings in Col4A1 Mutation AU - Yan Tong Koh AU - Conrad Schmoll Y1 - 2026/01/23 PY - 2026 N1 - https://doi.org/10.11648/j.wjmcr.20260701.11 DO - 10.11648/j.wjmcr.20260701.11 T2 - World Journal of Medical Case Reports JF - World Journal of Medical Case Reports JO - World Journal of Medical Case Reports SP - 1 EP - 4 PB - Science Publishing Group SN - 2994-726X UR - https://doi.org/10.11648/j.wjmcr.20260701.11 AB - Purpose: We aim to describe the fundal fluorescein angiography (FFA) findings in a patient with COL4A1 mutation which to date has not been described in this condition. We hope to highlight the variability in ocular phenotypes seen in COL4A1 mutation, even between eyes in the same patient. Methods: Case Report. Results: A 14 year-old girl with a history of cerebral palsy, cerebral visual impairment and COL4A1 mutation with porencephaly has been attending the eye service for bilateral aphakic glaucoma with previous bilateral glaucoma tube surgery on Latanoprost, Brinzolamide and Timolol to both eyes. She developed a spontaneous right vitreous haemorrhage and anterior chamber hyphaema, subsequently requiring a vitrectomy and anterior chamber washout due to elevated intraocular pressure. Intraoperatively, she was noted to have extensive ischemic changes in the right eye. In her left fundus, there were sclerosed arterioles emanating from the disc, with the rest of the retina being normal. Despite the vitrectomy, the right eye vitreous haemorrhage and hyphaema recollected over time with persistently high intraocular pressure. She underwent a repeat vitrectomy and washout, subsequent cyclodiode laser and evisceration after she developed a painful blind right eye. During the course of her treatment, a FFA for her left eye was performed. Delay in arm-retinal time and a “fern-leaf” pattern of capillary leakage was noted. Discussion: The disease resulting from COL4A1 mutation is extremely variable. We report a patient with COL4A1 mutation with asymmetric retinal pathology with one eye eventually needing evisceration. This case highlights the need to have a high index of suspicion for early detection and asymmetric disease. There should be a low threshold for further evaluation such as FFA or optical coherence tomography (OCT) angiography to evaluate for ocular perfusion. Although COL4A1 is a systemic disease, it can have asymmetric presentation between two eyes. VL - 7 IS - 1 ER -
National Healthcare Group Eye Institute, Tan Tock Seng Hospital, Singapore, Singapore;Royal Hospital for Children & Young People, NHS Lothian, Edinburgh, United Kingdom;Princes Alexandra Eye Pavilion, NHS Lothian, Edinburgh, United Kingdom
Royal Hospital for Children & Young People, NHS Lothian, Edinburgh, United Kingdom;Princes Alexandra Eye Pavilion, NHS Lothian, Edinburgh, United Kingdom
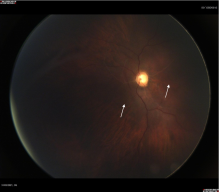
Figure 1. Left eye fundal photo: Sclerosed ghost-like arterioles emanating from the disc (labelled with arrow). Retinal venules were otherwise grossly normal with no retinopathy or ectatic vessels noted.
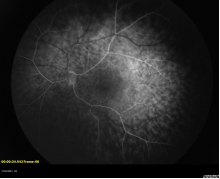
Figure 2. Left eye FFA: Delay in arm-retinal time with the arteriovenous phase at 34 seconds, with persistent patchy and mottled choroidal filling.
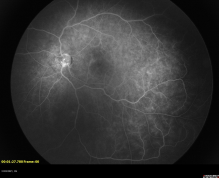
Figure 3. Left eye FFA: “Fern-leaf” pattern of capillary leakage and pinpoint areas of hyperfluoresence is visible in the temporal and inferotemporal quadrant.
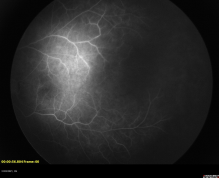
Figure 4. Left eye FFA: Twig-like abnormalities of retinal vasculature with no significant areas of peripheral ischemia or capillary fallout.
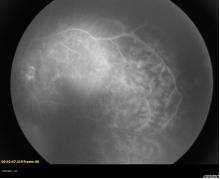
Figure 5. Left eye FFA: Late phase.

